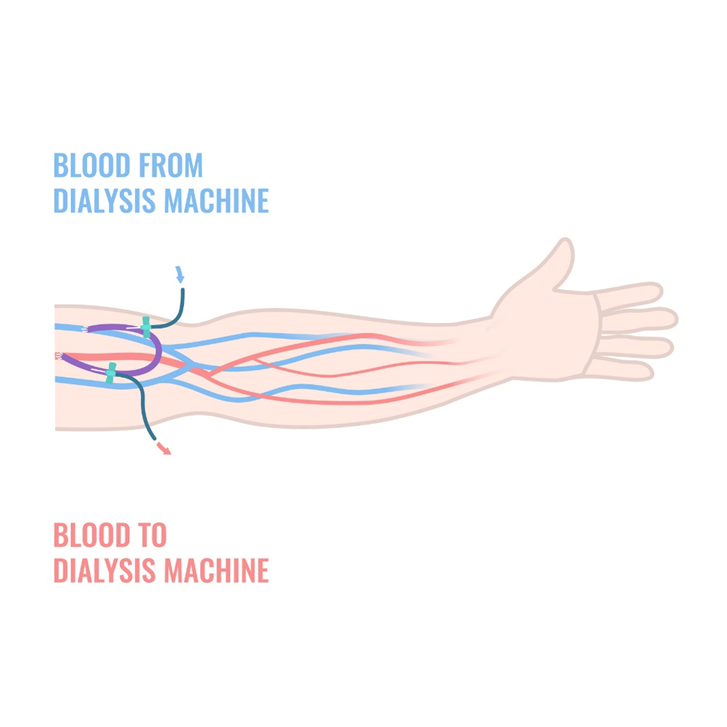
A fistula is a connection made between an artery and a vein. Arteries carry blood away from the heart under high pressure and veins return the blood to the heart under low-pressure. The surgically created join between the artery and vein causes an increase in the amount of blood flowing through the fistula vein. This creates the ideal location for accessing your blood for the dialysis machine.
An autologous fistula is created using your own vein and artery. The surgically created join is made as close to the hand as a patient’s anatomy will allow. The reason for this is that it reduces the risks of many of the known complications of AV fistulas. When an autologous fistula is first created the vein is not immediatly suitable for use by the dialysis machine. It often takes several weeks for the blood flow to increase to a level suitable for use by the dialysis machine. During this maturation period your fistula will be monitored with ultrasound scanning to ensure it is maturing appropriately.
A prosthetic fistula utilises a prosthetic graft that is tunnelled superficially under the skin to join between the vein and artery. The prosthetic graft is then used to provide access for the dialysis machine. They are reserved for patients who do not have suitable vessels to form an autologous fistula as they are more prone to infection and occlusion.
Permacath are commonly used for patients who commence dialysis in an urgent fashion without prior warning, and have not have time for a fistula to be formed. A permacath is a cannula placed into one of the main veins in your neck. This allows for immediate access for dialysis, however has the disadvantages of being quite prone to infection and occlusion. For this reason, the Australian kidney Association recommends where possible permacaths are only used on a temporary basis.
When you are referred to Dr McGlade by your renal physician he will take a thorough history and examination. He will organise an ultrasound scan to determine your most appropriate access for the dialysis machine. During the consult he will discuss with you your options for dialysis access as well as your future care plan for the fistula.